
As nicotine enters the body, it is distributed quickly through the bloodstream and crosses the blood–brain barrier reaching the brain within 10–20 seconds after inhalation.The elimination half-life of nicotine in the body is around two hours.The amount of nicotine absorbed by the body from smoking depends on many factors, including the types of tobacco, whether the smoke is inhaled, and whether a filter is used. For chewing tobacco, dipping tobacco, snus and snuff, which are held in the mouth between the lip and gum, or taken in the nose, the amount released into the body tends to be much greater than smoked tobacco.[clarification needed] Nicotine is metabolized in the liver by cytochrome P450 enzymes (mostly CYP2A6, and also by CYP2B6). A major metabolite is cotinine.
Other primary metabolites include nicotine N’-oxide, nornicotine, nicotine isomethonium ion, 2-hydroxynicotine and nicotine glucuronide. Under some conditions, other substances may be formed such as myosmine.
Glucuronidation and oxidative metabolism of nicotine to cotinine are both inhibited by menthol, an additive to mentholated cigarettes, thus increasing the half-life of nicotine in vivo.
Medical Detection
 Nicotine can be quantified in blood, plasma, or urine to confirm a diagnosis of poisoning or to facilitate a medicolegal death investigation. Urinary or salivary cotinine concentrations are frequently measured for the purposes of pre-employment and health insurance medical screening programs. Careful interpretation of results is important, since passive exposure to cigarette smoke can result in significant accumulation of nicotine, followed by the appearance of its metabolites in various body fluids. Nicotine use is not regulated in competitive sports programs.
Nicotine can be quantified in blood, plasma, or urine to confirm a diagnosis of poisoning or to facilitate a medicolegal death investigation. Urinary or salivary cotinine concentrations are frequently measured for the purposes of pre-employment and health insurance medical screening programs. Careful interpretation of results is important, since passive exposure to cigarette smoke can result in significant accumulation of nicotine, followed by the appearance of its metabolites in various body fluids. Nicotine use is not regulated in competitive sports programs.
Pharmacodynamics
Nicotine acts on the nicotinic acetylcholine receptors, specifically the ganglion type nicotinic receptor and one CNS nicotinic receptor. The former is present in the adrenal medulla and elsewhere, while the latter is present in the central nervous system (CNS). In small concentrations, nicotine increases the activity of these receptors. Nicotine also has effects on a variety of other neurotransmitters through less direct mechanisms.
In The Central Nervous System
By binding to nicotinic acetylcholine receptors, nicotine increases the levels of several neurotransmitters – acting as a sort of “volume control”. It is thought that increased levels of dopamine in the reward circuits of the brain are responsible for the apparent euphoria and relaxation, and addiction caused by nicotine consumption. Nicotine has a higher affinity for acetylcholine receptors in the brain than those in skeletal muscle, though at toxic doses it can induce contractions and respiratory paralysis. Nicotine’s selectivity is thought to be due to a particular amino acid difference on these receptor subtypes.
Tobacco smoke contains anabasine, anatabine, and nornicotine. It also contains the monoamine oxidase inhibitors harman and norharman. These beta-carboline compounds significantly decrease MAO activity in smokers.MAO enzymes break down monoaminergic neurotransmitters such as dopamine, norepinephrine, and serotonin. It is thought that the powerful interaction between the MAOIs and the nicotine is responsible for most of the addictive properties of tobacco smoking. The addition of five minor tobacco alkaloids increases nicotine-induced hyperactivity, sensitization and intravenous self-administration in rats.
Chronic nicotine exposure via tobacco smoking up-regulates alpha4beta2* nAChR in cerebellum and brainstem regions but not habenulopeduncular structures. Alpha4beta2 and alpha6beta2 receptors, present in the ventral tegmental area, play a crucial role in mediating the reinforcement effects of nicotine.
In The Sympathetic Nervous System
Nicotine also activates the sympathetic nervous system, acting via splanchnic nerves to the adrenal medulla, stimulates the release of epinephrine. Acetylcholine released by preganglionic sympathetic fibers of these nerves acts on nicotinic acetylcholine receptors, causing the release of epinephrine (and noradrenaline) into the bloodstream. Nicotine also has an affinity for melanin-containing tissues due to its precursor function in melanin synthesis or due to the irreversible binding of melanin and nicotine. This has been suggested to underlie the increased nicotine dependence and lower smoking cessation rates in darker pigmented individuals. However, further research is warranted before a definite conclusive link can be inferred.
In Adrenal Medulla
By binding to ganglion type nicotinic receptors in the adrenal medulla nicotine increases flow of adrenaline (epinephrine), a stimulating hormone and neurotransmitter. By binding to the receptors, it causes cell depolarization and an influx of calcium through voltage-gated calcium channels. Calcium triggers the exocytosis of chromaffin granules and thus the release of epinephrine (and norepinephrine) into the bloodstream. The release of epinephrine (adrenaline) causes an increase in heart rate, blood pressure and respiration, as well as higher blood glucose levels.
Nicotine is the natural product of tobacco, having a half-life of 1 to 2 hours. Cotinine is an active metabolite of nicotine that remains in the blood for 18 to 20 hours, making it easier to analyze due to its longer half-life.
Psychoactive Effects
Nicotine’s mood-altering effects are different by report: in particular it is both a stimulant and a relaxant. First causing a release of glucose from the liver and epinephrine (adrenaline) from the adrenal medulla, it causes stimulation. Users report feelings of relaxation, sharpness, calmness, and alertness. Like any stimulant, it may very rarely cause the often uncomfortable neuropsychiatric effect of akathisia. By reducing the appetite and raising the metabolism, some smokers may lose weight as a consequence.
When a cigarette is smoked, nicotine-rich blood passes from the lungs to the brain within seven seconds and immediately stimulates the release of many chemical messengers such as acetylcholine, norepinephrine, epinephrine, vasopressin, histamine, arginine, serotonin, dopamine, autocrine agents, and beta-endorphin.This release of neurotransmitters and hormones is responsible for most of nicotine’s effects. Nicotine appears to enhance concentration and memory due to the increase of acetylcholine. It also appears to enhance alertness due to the increases of acetylcholine and norepinephrine. Arousal is increased by the increase of norepinephrine. Pain is reduced by the increases of acetylcholine and beta-endorphin. Anxiety is reduced by the increase of beta-endorphin. Nicotine also extends the duration of positive effects of dopamine and increases sensitivity in brain reward systems. Most cigarettes (in the smoke inhaled) contain 1 to 3 milligrams of nicotine.
Research suggests that, when smokers wish to achieve a stimulating effect, they take short quick puffs, which produce a low level of blood nicotine. This stimulates nerve transmission. When they wish to relax, they take deep puffs, which produce a high level of blood nicotine, which depresses the passage of nerve impulses, producing a mild sedative effect. At low doses, nicotine potently enhances the actions of norepinephrine and dopamine in the brain, causing a drug effect typical of those of psychostimulants. At higher doses, nicotine enhances the effect of serotonin and opiate activity, producing a calming, pain-killing effect. Nicotine is unique in comparison to most drugs, as its profile changes from stimulant to sedative/pain killer in increasing dosages and use.
Technically, nicotine is not significantly addictive, as nicotine administered alone does not produce significant reinforcing properties. However, after coadministration with an MAOI, such as those found in tobacco, nicotine produces significant behavioral sensitization, a measure of addiction potential. This is similar in effect to amphetamine.
Nicotine gum, usually in 2-mg or 4-mg doses, and nicotine patches are available, as well as smokeless tobacco, nicotine lozenges and electronic cigarettes.
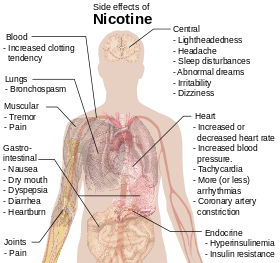
Side Effects
Nicotine increases blood pressure and heart rate in humans. Nicotine can also induce potentially atherogenic genes in human coronary artery endothelial cells. Microvascular injury can result through its action on nicotinic acetylcholine receptors (nAChRs).
A study on rats showed that nicotine exposure abolishes the beneficial and protective effects of estrogen on the hippocampus, an estrogen-sensitive region of the brain involved in memory formation and retention.